

Methandienone 10 mg/tb
Product Description
Drug name: Methandienone/Methandrostenolone
Drug class: Anabolic / androgenic steroids
Common drug quantity: Tablets: 5mg, 10mg, 20mg
Use and effective range:
Applications: muscle building, diet (conditional)
Anabolic components: strong
Androgenic components: strong
Dose range and duration of use:
Beginners: 10-15mg / day
Hobby: 15-45mg / day
Professional range: 45-100mg / day
Women: 5-15mg / day
Application period: 4-6 weeks
Active-Life: 6-8 hours (Injection product remains active for about
60-72 hours)
Drug Class: Anabolic/androgenic steroid
Average Reported Dosage: Men 15-100 mg daily Women 5-15 mg daily
Acne: Yes, especially in higher dosages.
Water Retention: Yes, similar to testosterone
High Blood Pressure: Yes, due to water retention, some experience
elevated heart rate
Aromatization: Yes, strongly
Liver Toxic: Yes, 17-alfa alkylated oral
DHT conversion: No
High anabolic/high androgenic
Decreases HPTA function: Yes, dose and administration period dependent
Description
Oral Dianabol was reported to be a highly effective mass AAS which provided impressive weight and strength gains. Most users experienced a 2-4 LB bodyweight increase per week with heavy water retention. With higher dosages gynecomastia (bitch tits) was a common negative side effect. Obviously much of this was avoided by those who reported co-addministration of Proviron and/or Novladex. When stacked with a nandrolone, some gyno problems seemed to lessen. This was probably due to Nandrolones aromatization to a weaker estrogen called Norestrogen and the resulting mild anti-estrogenic effect that results in moderate dosage administration. Methandrostenlone becomes active in 1-3 hours with a half-life of about 3.5-4.5 hours. For this reason, dosages were spread through out the day to maintain blood serum concentrations at an elevated state. Massive dosages just were not necessary since a single 10-mg dose has increase androgen anabolic activity 5 times over normal with a correlating reduction in natural cortisol activity of 50-70%. Males using 5mg per 25-LBS of body weight broken into 3-5 equal dosages throughout the day have experienced impressive results. At dosages above 50 mg per day, results were not progressively quantitative. Most first time AAS users who used a daily dosage of 20-30mg daily experience significant results over a 4-6 week period. Women should not utilize Methandrostenolone but a surprising number did report the inclusion of the drug in AAS protocols. For those who insisted, no more than 10-mg daily for 3-4 weeks stacked with a very low androgenic product minimized masculization type negative side effects. Side effects such as increased liver values (toxicity) “usually” returned to normal within a short period of time after use was discontinued. High blood pressure, elevated heart rates, gyno, heavy water retention, and acne were all frequent reported negative side effects of Methandrostenlone use. Some literature on this drug supports DHT- like activity. Finasteride “usually” prevented this effect as well as possible prostate enlargement. Dianabol heavily suppresses natural testosterone production within only 10 days after continuous administration begins (dose dependent). Most note a sense of well being during use of this drug. Significant strength and weight loss follows discontinued use due to the loss of excessive water and HPTA suppression. So retained gains were only fair post-cycle. My personal experiences with this drug have led me to believe that no athlete should have ever stacked high dosage protocols of Dianabol with Anadrol-50 or Methyltestosterone. It is a liver killer combo. A last note: Injectable Dianabol did not have anywhere Nera as dramatic effects when utilized in its intended method. However, the injectable is orally active and as such was reported to be commonly used in this manner by filling gel-caps with the desired amount/dosage and subsequent ingestion. This is probably due to the fact that oral administration of a c17-alkylated AAS results in increased liver production of IGF-1. I have also learned that it was best to avoid Russian Methandrostenlone. (It commonly contains a large amount of unconverted methyltestosterone).
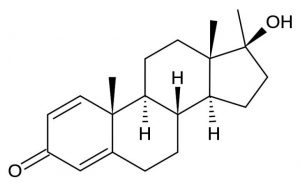
Structural Characteristics
Methandrostenolone is a modified form of testosterone. lt differs by: 1) the addition of a methyl group at carbon 17-alpha to protect the hormone during oral administration and 2) the introduction of a double bond between carbons 1 and 2, which reduces its relative androgenicity. The resulting steroid also has a much weaker relative binding affinity for the androgen receptor than testosterone, but at the same time displays a much longer half-life and lower affinity for serum-binding proteins in comprison. These features (among others) allow methandrostenolone to be a very potent anabolic steroid in spite of a weaker affinity for receptor binding. Recent studies have additionally confirmed that its primary mode of action involves interaction with the cellular androgen receptor.
Dosage Recommanded
Studies have shown that taking an oral anabolic steroid with food may decrease its bioavailability. This is caused by the fat-soluble nature of steroid hormones, which can allow some of the drug to dissolve with undigested dietary fat, reducing its absorption from the gastrointestinal tract. For maximum utilization,this steroid should be taken on an empty stomach.
The original prescribing guidelines for Ubolic called for a daily dosage of 5 mg.This was to be administered on an intermittent basis, with the drug taken for no more than 6 consecutive weeks.Thereafter, a break of 2 to 4 weeks was advised before therapy was resumed. For physique-or performance-enhancing purposes, the drug is also used intermittently, with cycles usually lasting between 6 and 8 weeks in length followed by 6-8 weeks off. Although a low dose of 5 mg daily may be effective for improving performance, athletes typically take much higher amounts. A daily dosage of three to six 5 mg tablets (15-30 mg) is most common, and typically produces very dramatic results. Some venture even higher in dosage, but this practice usually leads to a more profound incidence of side effects, and is generally discouraged. Ubolic stacks well with a variety of other steroids. lt is noted to mix particularly well with the mild anabolic Deca-Durabolin, for example. Together one can expect exceptional muscle and strength gains, with side effects not much worse than one would expect from Ubolic alone. For sheer mass, a long-acting testosterone ester like enanthate or cypionate can be used. With the high estrogenic/androgenic properties of this androgen. however, side effects should be more pronounced. Gains would be pronounced as well, which usually makes such an endeavor worthwhile to the user. As discussed earlier, ancillary drugs can be added to reduce the side effects associated with this kind of cycle. The half-life of Ubolic is only about 3 to 5 hours. A single daily dosage schedule will produce a varying blood level, with ups and downs throughout the day. The user, likewise, has a choice, to either split up the tablets during the day or to take them all at one time. The usual recommendation has been to divide them and try to regulate the concentration in your blood. This, however, will produce a lower peak blood level than if the tablets were taken all at once, so there may be a trade-off with this option. Both options work fine, but anecdotal evidence seems to support single daily doses as being better for overall results. With such a schedule, it seems logical that taking the pills earlier in the day would be optimal. This would allow a considerable number of daytime hours for an androgen-rich metabolism to heighten the uptake of nutrients, especially the critical hours following training.
Side Effects
All anabolic/androgenic steroids when taken in doses sufficient to promote muscle gain are expected to suppress endogenous testosterone production. Methandrostenolone is no exception, and is noted for its strong influence on the hypothalamic-pituitary-testicular axis. Clinical studies giving 15 mg per day to resistance-training males for 8 weeks caused the mean plasma testosterone level to fall by 69%. Without the intervention of testosterone-stimulating substances, testosterone levels should return to normal within 1-4 months of drug secession. Note that prolonged hypogonadotrophic hypogonadism can develop secondary to steroid abuse, necessitating medical intervention.